
‘When You Try to Stop It, Nothing Happens’: A Q&A on the History of Coerced Sterilization in California
"We should be critical about how we think of different groups and the way we justify treating different people," said Natalie Lira, one of the researchers urging California to pay reparations to the thousands of people coercively sterilized over the decades.
From 1919 to 1952, California coercively sterilized some 20,000 men and women, a disproportionate number of whom were of Mexican descent and often disabled or deemed “feeble-minded.” But unlike other states such as North Carolina and Virginia, California has yet to offer any reparations for sterilization survivors as a step toward confronting this injustice.
Last September, Alexandra Minna Stern, Nicole L. Novak, Natalie Lira, Kate O’Connor, Siobán Harlow, and Sharon Kardia published a thought-provoking article in the American Journal of Public Health documenting their research on the history of coerced sterilization in California and urging the state to “seriously consider reparations.” Their work is an interdisciplinary project bringing epidemiologists, historians, and Latinx and gender studies scholars together to explore a vast and complex topic.
Their research involved poring over decades of records, learning more about who was sterilized and why in institutional settings. These settings included Pacific Colony and Sonoma State Home, two institutions for “the feeble-minded”—a catchall term for people for people believed to have developmental disabilities or simply a history of criminality, promiscuity, or antisocial behavior—along with psychiatric institutions like Stockton State Hospital and Norwalk State Hospital, designated for people diagnosed as mentally ill. Stern and her colleagues digitized microfilm reels found in California’s Department of State Hospitals in Sacramento and used them to create a comprehensive data set. Some patients were recommended for sterilization after arrival, while others were specifically referred to institutions to be sterilized. These procedures were performed for eugenic purposes and, as detailed in a working paper based on the same data set, they were heavily informed by racism.
Stern, Novak, and Lira talked to Rewire about their research; what California should be doing for survivors of sterilization; and, critically, how we can prevent another wave of coerced procedures, both in California and in the rest of the United States.
Rewire: This is an insight into a dark period in California’s history. What was the catalyst for doing this research at this particular time?
Alexandra Minna Stern: Well, I think that there wasn’t really a particular catalyst; it was that I got to a point where the timing was right. And then we realized that to look at the entirety of the records, we had to create a data set. We’re fortunate to be here, at this university, where we could get pilot funding and work with willing and smart colleagues in epidemiology, one of who let us use her lab in the School of Public Health to do the data entry. For me, what’s been going on for the past several years is a long slog of getting the data entered and building up the research project. A lot of different students—undergrads, grad students from other departments, and now post-docs with [Novak]—are working on it. We’re in the position now where we can actually start using all of the data to start doing the quantitative and qualitative analysis.
I feel very committed to asking research questions that have social justice and disability justice and reproductive justice relevance. That, for me, is an inspiration, and we’ve been fortunate and have worked hard as a team to have received external and internal refunding. Without that funding, we wouldn’t have been able to do this. You can’t assemble a team if you aren’t able to compensate them.
Rewire: You released data on ethnic bias and sterilization in a working paper separate from the study. What racial trends of sterilization did you observe in your research, and how did that overlap with other targeting of marginalized populations?
Natalie Lira: One of the major trends that we found was that Mexican-origin patients were being targeted. Especially in the institutions that were housing people categorized as “feeble-minded”—in these cases, race and disability really worked kind of relationally. They were co-constructed.
So when I would look at the records of Mexican-origin women and men that were being sterilized, some of whom were immigrants, and many others of whom were first-generation Mexican-Americans, there was this very clear medical narrative where Mexican immigrants, and the idea of the Mexican race in general, were thought of as less intelligent and more prone to “feeble-mindedness,” according to a lot of studies published at the time. Because of this, they were seen as as inherently more prone to commit criminal acts; they were seen as lazy; Mexican women were seen as hyper-fertile and ignorant. There were these racial ideas about who Mexicans were, and who their children were. They played into this medical narrative of feeble-mindedness and cognitive disability. That was the main way that we saw race and disability kind of play together in the records.
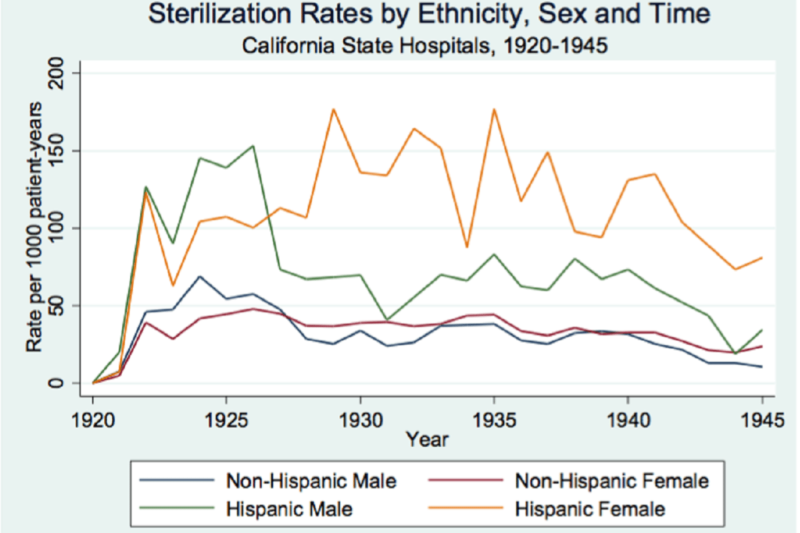
Nicole Novak: We were able to use Census records and look at, within people living in institutions, whether there was a higher risk of sterilization for people who had Spanish surnames, which approximates Latino identity, although not perfectly. Much like [Lira] observed in places like Pacific Colony, there was two to three times the risk of sterilization for people with Spanish surnames relative to people without. That kind of bias of higher risk of sterilization was greatest among those younger than 19, and also among women.
Rewire: While exploring your data, I was struck by the gender balance. Usually when we talk about sterilization, we focus on women, but you found that in California, the split was almost 50/50. Can you speak to that?
AMS: In broad national trends, when sterilization began as a eugenic policy in institutions across the country, it was initially more focused on men and vasectomies, in part because the operation was an easier one to perform. It was only later that the salpingectomy, a sterilization procedure in which the fallopian tubes are removed, was “perfected” by a physician at the Stockton Institution, Dr. Margaret Smyth. Over time, there was a shift, so that sometime in the 1930s nationally, it moved from more men being sterilized to more women being sterilized. And I think California mirrors that pattern pretty well.
However, in Southern states, they actually started their eugenics programs later. So for example, Georgia doesn’t pass its law legalizing eugenics until 1937. So by the time Georgia passes its law, targeting women was already the trend, and that also related to shifts in the way fitness and unfitness were understood.
Also, the trend of higher sterilization rates of women foreshadows what we see in the ’50s and ’60s with ideas around good mothers, the kinds of ideas that become so essential to the post-World War II welfare state. That’s why for example in North Carolina, by the end of the program in the 1960s, it’s primarily Black women being sterilized.
Eugenic ideas about degeneracy and unfitness morphed into concerns about “welfare queen” and undeserving mothers that increasingly began to affect women of color. It’s important to clarify that eugenicists were always worried about the burden or cost of “defectives” on public resources and society at large. This cost was seen as biological and economic. By the 1950s and 1960s, sterilization continues on in many states, because eugenics laws made sterilization legal practice, but the rationales have shifted away from primarily worries of eugenic fitness to concerns about irresponsible mothers who are not fit to parent. But in California, sometime around the late 1930s, that shift occurs where more women are being sterilized, and also there’s a relationship between being in a “feeble-minded” institution and being a woman and being sterilized.
Rewire: Did you encounter any specific cases over the course of your research that struck you as particularly horrific or startling?
NL: My specific knowledge is about one of the institutions for the “feeble-minded,” Pacific Colony, and I did go through the majority of those records one by one. There were so many different cases over the period of time from 1927 to 1952. There were cases of young women who were victims of rape and then accused of being promiscuous. Young men charged with petty crimes like theft of property, or simply acting out, they would get sent to these institutions and sterilized. There are so many cases.
What became very clear going through these cases is how lower-class, racialized communities were under a microscope. Their lives were being policed and examined, their sexual acts, their intimate household lives, their family formations. They were placed under extreme scrutiny and pathologized. Especially in the cases of young Mexican-American women and men, they were not allowed social transgressions at all. Expressions of sexual agency in young women, or rebellion in young men, they weren’t painted as youthful mistakes. They were really read as mental deficiency and potential social threat, so they often sustained harsher punishments than white youth. There were also a lot of cases where youth that were orphaned, through no fault of their own, were dropped in the juvenile system, and became wards of the state. They weren’t able to be in orphanages because they acted out, so they were sent to institutions.
AMS: One of the things we see particularly with Mexican-origin patients is that sibling groups would be committed and often sterilized. There was this assumption that if one of the kids was “defective” in some way, that the brothers or sisters would be too. I’ve seen many instances where the documentation says: “Brother at Stockton, sister at Pacific Colony.” That undergirds the idea that Mexicans as a community were being racialized and medicalized. And you can see that in the way families were pathologized and ultimately disarticulated because the family members are being sent to different places. Parents often had little recourse to change the situation.
In a case I came across recently, and this was the first case that I found of someone who appeared to be transgender; we’ll call her “Martina Ruiz.” Martina was really born with the anatomy of Martino. She was actually treated as female in all of the doctors’ records, but then was pathologized as a sexual delinquent. I think that there’s a lot of sexual policing that was going on. That does connect to disability discourses, because almost everyone in this institution was viewed as “less-than” somehow.
Rewire: Are there any stories that you feel aren’t being told?
AMS: We were contacted by a researcher looking back at “mental retardation” in San Francisco in the mid-century. She interviewed the kinds of psychologists who were giving IQ tests to people who would be sent to places like Sonoma State Home. She learned about cases along the way of women who wanted sterilization, and so they were okay with being labeled as mentally deficient because that was the only route to permanent birth control. That’s something that Johanna Schoen saw: 5 percent of North Carolina records were women who voluntarily went to the county eugenics board so that they could get permanent birth control. So I think that often gets left out. The narrative of eugenics as only victimization then elides the fact that sterilization was occasionally a desired, and often elusive, form of birth control during this time period.
We really want this project to be situated around reproductive justice and access to the full spectrum of reproductive decision making that women need, want, and deserve. This makes the conversation messier, but reflects the fact that some women didn’t have access to sterilization because of the way things were at the time. I don’t know if there’s a way we can tell from the documents, but that is probably part of this story. Often in the narrative, especially when people sensationalize the narrative, that part, that sterilization is an integral part of women’s reproductive health, is often lost.
NL: That can be read in some of the cases. Especially when I was looking at Pacific Colony, I did come across a small number of records where it seemed as though the person was not institutionalized, but just sent to the institution for the operation. That’s how I would sometimes read those cases. There were not many.
Rewire: The story of sterilization in California often feels hidden from the mainstream. Do you have any theories about what’s causing this?
NL: This is something that all of us have thought about, and even when we were writing that article, that was a question. In North Carolina, the push for reparations largely came from survivors of sterilization. That hasn’t really happened in California yet. A lot of it has to do with the shame and the fear and the remaining after effects of the feeling that comes from being pathologized and placed in an institution and subjected to an operation. Even people that have come forward and talked to us have specifically mentioned that their family members haven’t wanted to talk about it because there’s a lot of shame. There are associations with being diagnosed as mentally ill and placed in an institution.
AMS: It’s a fascinating question. What’s interesting is that as we’ve talked to more people, and specifically family members, those words themselves—shame, pain, secrets—those words come up over and over again. That’s definitely part of the dynamic at play. Another issue is that California passed one of the first laws in the country, and most of the operations took place from the 1920s to the 1950s. By 1953, they had started to taper off (because of a modification to the law which made the process more involved, requiring more steps), though they did not stop completely, at least under the eugenics law, until the repeal in 1979. We’re looking at an older demographic group of patients than in North Carolina and Virginia.
I’ve thought a lot about this because I’m very interested in figuring out the approaches to take if we’re able to work with the state to go about identifying some of the living victims. That requires knowing something about who they are and where they might be now. I learned that in North Carolina, one of the ways they looked for victims was, by that time in the ’50s and ’60s, women being sterilized had received welfare or were hooked into bureaucracy; their name was in some state system somewhere. In California, it’s really different, because all we know is that they were in these institutions in these particular years. How do you go about finding these affected communities?
This has prompted me to think a lot about community. It seems like in Virginia and North Carolina, and Oregon—where in the latter there haven’t been reparations, but there has been an apology—there was some sense of collectivity or being part of a wronged social group. In California, the program ended up atomizing people to such a degree that people haven’t found each other after the fact. There’s not a sense of community identification. Hopefully, our work can create a space for that kind of identification, without the shame, recognizing that people were wronged by the state and should rightfully get some recognition and not be ashamed to talk about what happened to them. In California, people were in institutions all over the state. Looking through these 20,000 records and the stories that I know, there was real fragmentation.
NL: I agree, and it’s not to say that people don’t speak up about what happened to them. I look at a lot of cases where people were sentenced to institutions and were going to be sterilized, and family members brought legal cases, sought allies, and wrote letters. It’s not to say that everyone was silent about it or just let it happen and forgot about it. But a lot of the time people would try to prevent it from happening and it would happen anyway, so I think that also created a sense of: “What’s the point of bringing this up again?” One of the cases that we looked at and talked about a lot was Sara Rosas Garcia v. Department of Institutions (1939). She was a single mother and a widow with nine kids total who had very few resources, and her daughter was going to be sent to an institution and sterilized. She sought pro bono legal assistance and they brought a case to court. The same day, the case was thrown out: Her daughter was sterilized anyway. That created a sense of hopelessness and distrust not only in the medical establishment, but the law. Where do you go? Who do you talk to? When you try to stop it, nothing happens.
It should be noted that it’s not that there was complete silence and people didn’t do anything. There was also a case where a young woman sued the state hospitals after being sterilized.
AMS: There was resistance, particularly among Mexican origin families, who were the most vocal, probably for a variety of reasons. It’s really important to document that resistance and connect it to the history of reproductive justice in California. It’s interesting, if you think about the Frontline “No Más Bebés” documentary, part of the process was creating a safe space for the plaintiffs, many of whom hadn’t spoken about what had happened to them for decades, many of whose family members just learned about it during the documentary, and one of the plaintiff’s sisters didn’t even know about it until she went to the debut. She was stunned about what had happened to her sister. The filmmakers there did this amazing job. The community engagement and activism around that documentary is creating a safe space, where the women could reunite and feel that solidarity. That’s something I’m thinking a lot about as we’re being contacted by people and seeing maybe something happening around compensation and redress. I want to do that in a way that is informed by really good values.
Rewire: As the recent case in the California prison system reminded us, coerced sterilization is not a thing of the past—and there were no reparations given in that case. What kinds of factors need to coalesce to create these pockets of contemporary sterilization abuse?
NL: There are a lot of similar discourses at play. These women were criminalized, seen as deviant, and also charged as being dependent on the state. When you paint populations and individuals as being deviant, dependent, and unworthy, you also construct them as undeserving of rights. They’re already being warehoused. There are a lot of similar ideas at play. These are poor communities, often communities of color, and they are supposedly undeserving of the same rights because they’re already in prison; they’ve proven that they’ve done something wrong. In this framework, they are not worthy of parenthood, they’re not worthy of control over their bodies. We should be critical about how we think of different groups and the way we justify treating different people.
AMS: There’s a similar dehumanization at play in both of those institutions. One of the things Nicole did for us was showing trans-institutionalization. As mental institutions were shuttered and so many people who were held for many years in the ’70s and ’80s in California were released, by the ’80s and ’90s, you get rising rates of incarceration. It’s not the exact same person who goes from Stockton to the Corona Prison, but it’s a similar demographic of people—often people of color, poor people, people who are brought in on the first offense, or on three strikes, minimum sentencing laws.
One of the things you had with the institutions during the era that we studied was a real lack of accountability. The sterilization law accorded a lot of authority to the superintendents, and they could proceed unabated. Even if a family member or a patient said: “I reject the operation, I don’t want to be sterilized,” the law gave them the authority to override that. That was also enhanced by their medical authority, and in that setting, it was really paternalistic. They could just override any resistance or outright refusal of sterilization. At these total institutions, as I call them, superintendents could largely do what they wanted until the 1950s. In the California prisons, you have a similar lack of accountability. It’s a troubled public system that is accompanied by an increasingly privatized outsourcing of certain functions.
We know California is one of the most progressive states. It’s the bluest state at this point. It’s the state that’s going to take on Trump. I find it really fascinating that in California, one of the few states where you have people elected because they are talking about things like social justice and LGBTQ rights, and community activism, especially in urban areas, you have a prison system like that. It’s a state where we’ve seen these repeated episodes of sterilization abuse. Now, the prison situation: The response to that was swift, and soon after that an audit was done and a law was passed banning sterilization in state prisons except in extreme medical circumstances.
One of the things I feel strongly is that given California’s own progressive values, of all the states, it’s the state that should be committed and interested in looking back at this past, trying to look at what went wrong—what was the perfect storm that allowed all this to happen—and in finding individuals who were wronged and finding a way to recognize them and maybe even compensate them. I continue to be surprised by a variety of things around this incongruous nature of California.
CORRECTION: This article has been updated to clarify the proportion of people coercively sterilized who were of Mexican descent.